Prolapse Uterus
Prolapse Uterus
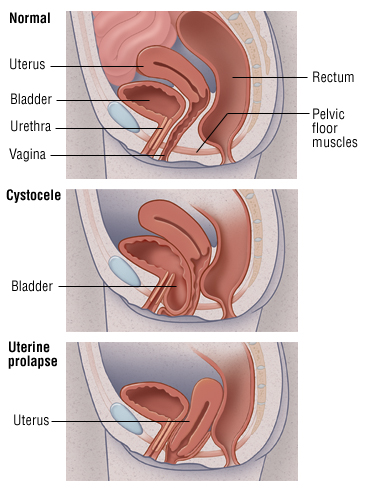
Uterine Prolapse is when the uterus descends towards or through the opening of the vagina.
The descent of the uterus and the vagina from its normal position is known as prolapse. The cause of prolapse is difficult to understand without knowledge of the anatomy of the pelvic floor and the ligamentary supports of the uterus and the vagina.
Chief Supports of the Uterus
- Condensations of endopelvic fascia-
- Uterosacral ligament,
- Transcervical (Mackenrodti’s) ligaments, and
- Pubo cervical ligament.
2. Pelvic diaphragm formed by the levator ani muscle.
3. Perineal body and the superficial perineal muscles.
The vagina is mainly supported by the vaginal sheath which is a part of the visceral pelvic fascia, and the muscles of the pelvic floor.
Etiology
Injury during child birth is generally implicated as the most important factor, but sufficient emphasis must also be given to musculofascial atony which occurs and increases after menopause.
Predisposing Factors
- Congenital or developmental weakness of the supports of the uterus- It causes a nullipaorus type of proplapse. Congenital weakness of supports of uterus is evidenced by a history of easy labours and strong familial incidence. It may be seen in young virgins with spina bifida occulta and split pelvis. The vaginal portion of the cervix is elongated and is the differentiating feature from acquired prolapse where the supra vaginal portion of the cervix elongates. There is no cystocoele or rectocoele. The term nulliparous is a misnomer as this type of prolapse may also be seen in multiparas and after menopause.
- Obesity.
- Chronic coughing or straining.
- Chronic constipation.
2. Acquired
- Childbirth injuries- The delivery of a child results in injury to the uterosacral and cardinal ligaments, larceration and separation of the levator ani and perineal muscles and thus causes weakness of the uterine supports. Prolonged distention or overstretching of the vagina in the second stage of labour causes stretch and weakness of the vaginal sheath and results in the vaginal wall prolapse. The application of forceps before full dilation of the cervix, unrepaired tears or larceration of the perineal body and passage of a large baby through the birth canal will also predispose to prolapse.
- Inadequate puerperal rehabilitation.
- Rapid succession of pregnancies when the tissues do not regain their original tone before the next pregnancy occurs.
- Atrophy of supporting tissues at the climacteric due to lack of oestrogens.
- Poor abdominal musculature leads to visceroptosis.
Degree of Uterine/Uterovaginal Prolapse (Malpas Classification)
First Degree- The descent of the uterus into the vagina upto the introitus.
Second Degree- The cervix protrudes through the introitus to a varying degree the fundus of the uterus is still in the vagina.
Third Degree- The entire uterus comes below the introitus. The whole vagina or at least its anterior wall is inverted. This is also described as procidentia.
Symptoms
- Discomfort
- Pain in the pelvis, abdomen or lower back
- Pain during sex
- Discharge
- Backache
- Urinary symptoms
- Rectal symptoms
Treatment
Palliative- It is done in situations where surgery is not advisable as in pregnancy, puerperium, or in women with severe medical disorders which contraindicate surgery. A ring pessary made of polyethylene is preferred over contraindicated surgery. The correct size of the pessary is the largest size which the patient can tolerate without discomfort, and of which she is unaware after wearing. The pessary is compressed into an ellipse and guided through the introitus. The index finger guides the upper end in the posterior fornix so that cervix lies in the ring and the anterior end is allowed to rest above the pubic symphysis. After insertion the patient is asked to strain to see if the pessary remains in position. The patient is advised to take vaginal douche and come for regular check-up and change of pressary after every three months. The long-term use of pessaries can lead to extensive vaginal discharge, vaginal ulcerations and even carcinoma. Hence the pessary cannot be used as a permanent cure.
Operative Treatment
Preoperative Assessment- General health of the patient is evaluated. Any existing predisposing factors are treated prior to surgery, coexisting urinary tract infection is treated.
The type of operation for prolapse depends on individual features. There is no fixed and the choice of operation is based on the age of the patient, parity, presence of associated abnormalities and the type and degree of prolapse.