Episiotomy
Episiotomy
An episiotomy is the surgical incision made to enlarge the vaginal opening for delivery of the baby’s head. An episiotomy involves incision fourchette, the superficial muscles and skin of the perineum and the posterior vaginal wall.
It is an incision made into the thinned out perineal body to enlarge the vaginal orifice during delivery.
Types of Episiotomy
Median
The incision begins in the centre of the fourchette and is directed posteriorly for approximately 2.5 cm in the midline of the perineum.
Advantage:-
- Less bleeding
- More easily and successfully repaired
- Greater subsequent comfort for the women
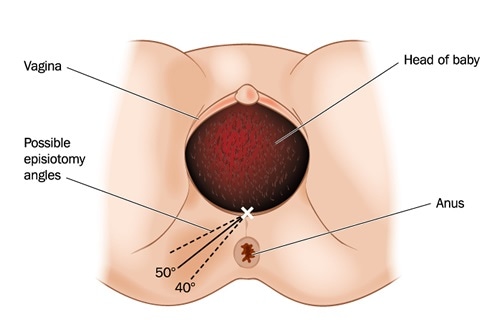
Medio lateral
The incision begins in the centre of the fourchette and is directed posteriorly, i.e. made diagonally in a straight line, 2.5 cm away from the anus, i.e. at 7 o’clock position, if the anus is considered to be at 6 o’clock position.
Advantages
- barthlion glands are not affected
- Anal sphincters are not injured
![]()
J-shaped
The incision begins in the centre of the fourchette and is directed posteriorly along the midline for about 1.5 centimetres(.59in) and then directed downwards and outwards along the 5 or 7 o’clock position to avoid the internal and external anal sphincter. This procedure is also not widely practiced.
Disadvantage
- The suturing is difficult
- Shearing of the tissue occurs
- The repaired wound tends to be pucked.
Lateral
The incision is begun one or more cm distant from the centre of the fourchette.
This incision starts about 1cm(0.4in) away from the centre of the fourchette and extends laterally. Drawbacks include the chance of injury to the Bartholin’s duct; therefore, some practitioners have strongly discouraged lateral incision.
Disadvantages
- Bartholins duct may be served
- The levatorani muscle is weakened
- Bleeding is more profuse
- Suturing is more difficult
- The woman experiences subsequent discomfort
Timing of Episiotomy
The episiotomy has to be performed timely, when the perineum is bulging and 3-4 cm diameters of the fetal scalp is visible during a contraction. If episiotomy is performed early, it will fail to release the presenting part and there can be haemorrhage from cut vessels. If it is performed late, the procedure fails to prevent laceration and to protect the pelvic floor.
Indications
- Maternal- Rigid perineum disproportion between foetus and vaginal orifice.
- Foetus- Cord prolapse in second stage, preterm baby.
- Others-For vaginal or intrauterine manipulation, e.g. forceps and breech delivery.
Advantages
- Reduction of foetal hypoxia and acidosis.
- Reduction in overstretching of the perineum
- Bruising of urethra is avoided
- Reduction in bearing down effort in conditions like preeclampsia and cardiac diseases.
- Prevention of third-degree tear, in case of presence of scar tissue, which does not stretch, well.
Perineal Lacerations
Perineal lacerations usually occur as the head is being born. The perineum elongates and thins out and is liable to tear. The extent of the laceration is defined on the basis of the depth.
- First degree- Laceration extends through the skin and structures superficial to muscles; the fourchette only is torn.
- Second degree- Laceration extends through muscles of perineal body; it is beyond the fourchette, but does not involve rectum or anus.
- Third degree- Laceration continues the anal sphincter muscle.
- Fourth degree- Laceration also involves the anterior rectal wall.
Layers to be repaired
1. Vaginal wound
- Deep and superficial tissue
- Vaginal mucosa
2. Perineal muscles and fascia
3. Perineal skin and subcutaneous tissue
4. The first stitch inserted at the apex of the incision
The most commonly used suturing material is 2/0 chromic catgut.
Signs that the perineum is liable to tear-
- Perineum does not stretch; resists the pressure of the descending head.
- A long perineum; appears oedematous
- Trickling of blood from the vagina (due to laceration of the vaginal mucous on the inner surface) when the head is on the perineum.
- Bluish appearance in the midline of the perineum, which later becomes white, shiny and transparent.
Prevention of Perineal Tears
- Principle of management of the second stage of labour should be that the smallest possible diameter of the head and shoulders should be permitted to emerge and distend the vulva.
- Encourage woman to take deliberate breaths through her mouth without accentuating expiration. This inhibits the desire to push when the head is distending the perineum.
- Midwife to have control of the advancing head, by placing finger tips on or near the head to restrain it.
- Maintain flexion and controlling too rapid extension of the head in vertex presentation.
- Prevent/active extension before crowing; prevent sinciput from gliding over the perineum until the occipital prominence and if possible, the parietal eminencies have been born.
- Keep hands off the perineum: Pressure of the fingers on the perineum further thins the perineum and causes bruising which favours tearing.
- Deliver the head at the end of or between contractions.
- Allow the woman to ‘breathe the head out’.
- While delivering the shoulders ensure that they have rotated internally, if not they will rotate while passing through the vulva, causing strain on the perineum.
Remember:
- Do not tie the sutures too tightly
- The last stitches are important for they prevent excessive scar.
- Press firmly on suture line with a pad to see if bleeding has stopped.
- Remove perineal pad or suture pack from vagina. Rub up fundus put clean pad on perineum
- Put gloved finger in to the rectum – to make suture that no stitch has one through the rectum
- Make the women comfortable, clean and dry.
After care of episiotomy
- Hot bath, clean wound care
- If pus or fouls smelling discharge develop report to health personnel.
- Advise not to strain and avoid constipation.