Physiological changes in the first stage
NORMAL LABOUR
Defintion- Labour is described as the process by which the fetus, placenta and memberane are expelled through the birth canal.
Normal labour occurs at term and is spontaneous in onset with the fetus presenting by the vertex. The process should be completed with acceptable time with in 24 hours vaginally. With no complications arise.
Definition
The physiological process by which the fetus, placenta, and membranes are expelled through the birth canal. The first stage of labour is from the onset of regular uterine contractions until full dilatation of the cervix.
Physiological changes in the first stage-
The onset of labour is a process, not an event. Cervical ripening takes
place from 36 weeks’ gestation.
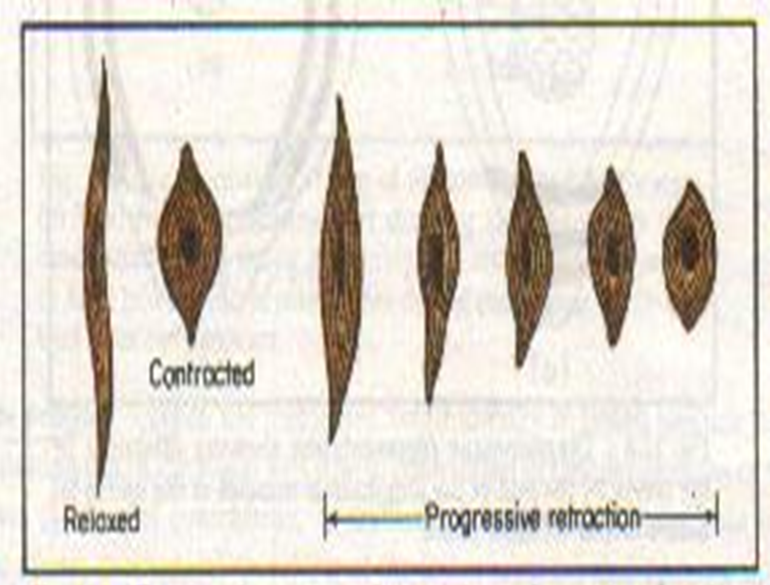
- Contraction and retraction- Shortening of the uterine muscles occurs with every contraction, mainly in the upper segment. Progressive pull on the weaker lower segment results in effacement and dilatation of the cervix. The latent phase of the first stage is considered to be up to 3cm, whilst the active phase is from 3cm to 10cm.
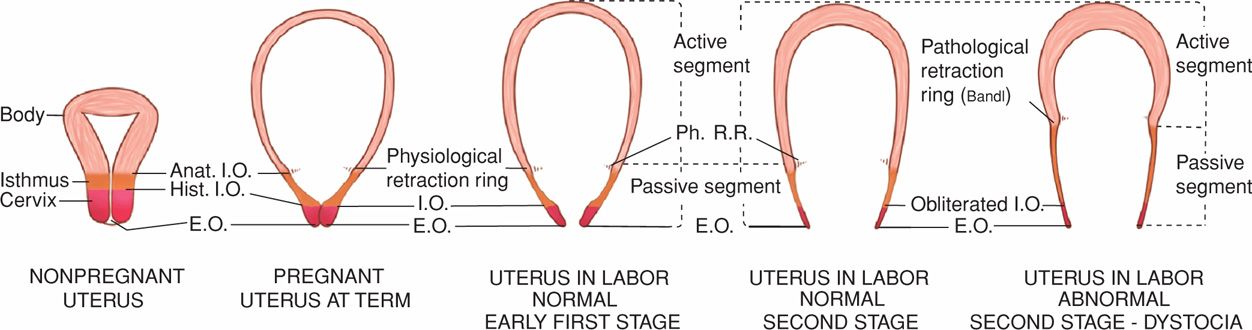
- Retraction ring- A normal occurrence in all labours. Ridge formation occurs between the thick, retracted muscles of the upper segment and the thin, distended aspect of the lower segment. Only visible in obstructed labour, when a transverse ridge across the abdomen forms — known as Bandl’s ring — indicates imminent rupture of the uterus.
- Fundal dominance- Contractions commence from the cornua and pass in waves in an inwards and downwards direction. Intensity of uterine action is greater in the upper segment.
- Upper active segment/lower passive segment- Shortening of the upper segment exerts pull on the passive lower segment. This initiates a reflex releasing oxytocin via the posterior pituitary, and assists with effacement and dilatation.
- Polarity of the uterus- Coordination between upper and lower segments; a balanced, harmonious and rhythmical process. The upper segment contracts powerfully and the lower contracts slightly and dilates.
- Resting tone- During a contraction the blood flow to the placenta is impaired so that oxygen and carbon dioxide exchange in the intervillous spaces is reduced. The resting tone is the relaxation period between contractions which enables placental blood flow to resume normal levels, to ensure adequate fetal oxygenation. The uterus is never completely relaxed; the measurement of the resting tone is 4–10mmHg.
- Intensity of contractions- Contractions cause a rise in intrauterine pressure (amplitude), which can be recorded. Contractions rise rapidly to a peak, then slowly diminish (resting tone).
- Early labour, > 20mmHg, 20–30s every 20min.
- Established labour, > 60mmHg, 45–60s every 2–3min.
- Formation of forewaters and hind waters- The result of the descent of the fetal head on to the cervix, which separates a small bag of amniotic fluid in front of the presenting part. The forewaters assist effacement of the cervix and early dilatation. The hindwaters fill the remainder of the uterine cavity; they help to equalize pressure in the uterus during contractions, thus providing protection to the fetus and placenta.

- Rupture of the membranes- Is thought to occur as a result of increased production of PGE2 from the amnion during labour, together with the force of the contractions. In a normal labour without intervention, the membranes usually rupture between 2cm and 3cm, around full dilatation or in the second stage.
- Show- Displacement of the operculum as a result of effacement and dilatation of the cervix. This can occur at any time during labour, but more commonly towards the end of the first stage or at full dilatation. Sometimes a show may occur before the onset of labour, however, this is not an indication that labour is apparent.
- Fetal axis pressure- This is the force transmitted by the uterine contractions down the fetal spine to its head.