True labor pain&False labor pain
Terminology-
✔️Multipara -is one who has completed two or more pregnancies to the stage of viability or more.
✔️ A primigravida is one who is pregnant for the first time.
✔️A nulligravida is one who is not now and never has been pregnant.
✔️A parturient is a women in labor.
✔️A multigravida is one who has previously been pregnant. She may have aborted or have delivered a viable baby.
✔️A primipara is one who has delivered one viable child. Parity is not increased even if the fetuses are many (twins, triplets).
✔️A nullipara is one who has never completed a pregnancy to the stage of viability. She may or may not have aborted previously.
✔️A puerpera is a woman who has just given birth.
✔️Ultrasound examination between 16 and 20 weeks is done to assess accurate gestational age, to detect fetal abnormality, viability and multiple pregnancy.
✔️Fetal movement count by the mother is an ideal first-line screening test both for high-risk and low-risk patients. A healthy fetus should have minimum 10 movements in 12-hour period. Count should be done daily beginning at 28 weeks. Mothers perceive 88% of fetal movements detected by sonography.
✔️Fetal cardiac accelerations- are associated with fetal movements in more than 85% of the time. A reactive NST requires at least two accelerations of FHR in 20 minutes of monitoring.
✔️False Pain (Synonym-false labor, spurious labor)- It is found more in primigravidae than in parous women. It usually appears prior to the onset of true labor pain by 1 or 2 weeks in primigravidae and by a few days in multiparae. Such pains are probably due to stretching of the cervix and lower uterine segment with consequent irritation of the neighboring ganglia.
✔️ Prelabor(Synonym: premonitory stage)-The premonitory stage may begin 2–3 weeks before the onset of true labor in primigravidae and a few days before in multiparae. The features are inconsistent and may consist of the following:
✔️ “Lightening”- A few weeks prior to the onset of labor especially in primigravidae, the presenting part sinks into the true pelvis. It is due to active pulling up of the lower pole of the uterus around the presenting part. It signifies incorporation of the lower uterine segment into the wall of the uterus. This diminishes the fundal height and hence minimizes the pressure on the diaphragm .The mother experiences a sense of relief from the mechanical cardiorespiratory embarrassment. There may be frequency of micturition or constipation due to mechanical factor—pressure by the engaged presenting part. It is a welcome sign as it rules out cephalopelvic disproportion and other conditions preventing the head from entering the pelvic inlet.
✔️ Cervical changes: A few days prior to the onset of labor, cervix becomes ripe. A ripe cervix is
- Soft,
- 80% effaced (<1.5 cm in length),
- Admits one finger easily, an
- Cervical canal is dilatable.
Appearance of false pain.
True labor pain is characterized by-
- Painful uterine contractions at regular intervals,
- Frequency of contractions increase gradually,
- Intensity and duration of contractions increase progressively
- Associated with “show”,
- Progressive effacement and dilatation of the cervix,
- Descent of the presenting part,
- Formation of the “bag of forewaters” and
- Not relieved by enema or sedatives.
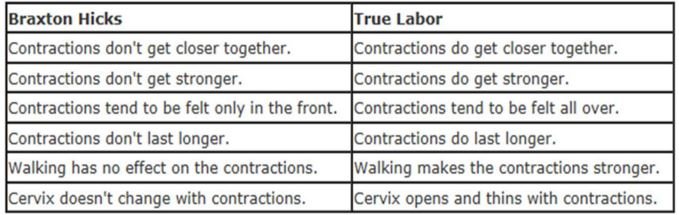
False labor pain is(Braxton Hicks)- contractions, also known as prodromal labor or practice contractions, or false labor, are sporadic uterine contractions that sometimes start around six weeks into a pregnancy.
- Dull in nature
- Confined to lower abdomen and groin
- Not associated with hardening of the uterus
- They have no other features of true labor pain as discussed above and
- Usually relieved by enema or sedative.